During change-of-shift report, a nurse discovers they overlooked a prescription for a type and cross-match of a client who is to have surgery the next day. Which of the following actions should the nurse take first?
Inform the provider of the delay in obtaining the type and cross-match.
Document the incident in the client’s medical record.
Prepare an incident report for risk management.
Obtain the client’s type and cross-match.
The Correct Answer is D
Choice A Reason:
Informing the provider of the delay in obtaining the type and cross-match is important for keeping the healthcare team informed. However, this action should follow the immediate step of obtaining the type and cross-match to ensure the client has compatible blood available for surgery. Communication with the provider is crucial but secondary to addressing the immediate need.
Choice B Reason:
Documenting the incident in the client’s medical record is necessary for maintaining accurate records and ensuring continuity of care. However, this action should be performed after the immediate need for obtaining the type and cross-match is addressed. Accurate documentation is essential but not the first priority in this situation.
Choice C Reason:
Preparing an incident report for risk management is important for identifying and addressing potential system issues that led to the oversight. However, this action is not the immediate priority. The primary focus should be on obtaining the type and cross-match to ensure the client’s safety during surgery. Incident reporting can be done after the immediate needs are met.
Choice D Reason:
Obtaining the client’s type and cross-match is the first action the nurse should take because it ensures that the client will have compatible blood available for transfusion if needed during surgery. This step directly addresses the immediate clinical need and prioritizes the client’s safety and readiness for surgery.
Free Nursing Test Bank
- Free Pharmacology Quiz 1
- Free Medical-Surgical Quiz 2
- Free Fundamentals Quiz 3
- Free Maternal-Newborn Quiz 4
- Free Anatomy and Physiology Quiz 5
- Free Obstetrics and Pediatrics Quiz 6
- Free Fluid and Electrolytes Quiz 7
- Free Community Health Quiz 8
- Free Promoting Health across the Lifespan Quiz 9
- Free Multidimensional Care Quiz 10
View Related questions
Correct Answer is C
Explanation
Choice A Reason:
The four-point alternating gait is used when a client can bear weight on both legs. This gait provides maximum stability and is often used for clients with poor balance or coordination. It involves moving one crutch forward, followed by the opposite leg, then the other crutch, and finally the other leg. Since the client can only bear weight on one leg, this gait is not appropriate.
Choice B Reason:
The two-point alternating gait is also used when a client can bear weight on both legs. It is faster than the four-point gait and involves moving one crutch and the opposite leg simultaneously, followed by the other crutch and the opposite leg. This gait requires partial weight-bearing on both legs, making it unsuitable for a client who can only bear weight on one leg.
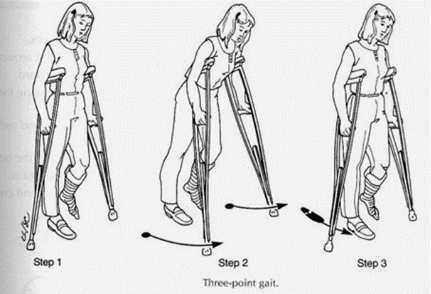
Choice C Reason:
The three-point gait is specifically designed for clients who can only bear weight on one leg. In this gait, both crutches are moved forward together, followed by the weight-bearing leg. The non-weight-bearing leg is then swung through. This gait provides the necessary support and stability for clients with one non-weight-bearing leg, making it the most appropriate choice in this scenario.
Choice D Reason:
The swing-through gait is used by clients who have good upper body strength and can bear weight on both legs, even if one leg is weaker. This gait involves moving both crutches forward together and then swinging both legs through to the crutches. It is not suitable for a client who can only bear weight on one leg, as it requires some degree of weight-bearing on both legs.
Correct Answer is D
Explanation
Choice A Reason
Allowing the client to hear running water while attempting to void can sometimes help stimulate urination through the power of suggestion. This method is non-invasive and can be effective for some patients. However, it may not be sufficient for a client who is 6 hours postoperative and experiencing significant difficulty voiding. In such cases, more direct intervention may be necessary to prevent complications like bladder distension or urinary retention.
Choice B Reason
Encouraging fluid intake up to 1,000 mL daily is generally good advice for maintaining hydration and promoting urinary function. However, in the immediate postoperative period, especially within the first 6 hours, the focus should be on addressing the acute issue of urinary retention. Increasing fluid intake alone may not resolve the problem and could potentially exacerbate bladder distension if the client is unable to void.
Choice C Reason
Providing the client a bedpan while lying supine is a practical approach to assist with urination, especially if the client is unable to get out of bed. However, the supine position is not the most conducive for voiding, as it can make it more difficult for the bladder to empty completely. This method might not be effective for a client experiencing significant difficulty voiding postoperatively.
Choice D Reason
Inserting an indwelling urinary catheter and connecting it to gravity drainage is the most appropriate action for a client who is 6 hours postoperative and having difficulty voiding. This intervention directly addresses the issue of urinary retention by ensuring that the bladder is emptied, thereby preventing complications such as bladder distension, urinary tract infections, and potential kidney damage. It is a standard practice in postoperative care when less invasive methods are ineffective.