A nurse is caring for a client whose family member requests to view the client’s medical record. Which of the following responses should the nurse make?
The ethics committee will need to approve this request for you.
I will ask the nursing supervisor to obtain the medical records for you.
The healthcare provider will share this information with you.
The client must provide permission to share the records with you.
The Correct Answer is D
Choice A reason:
The ethics committee does not typically handle requests for access to medical records. Their role is more focused on addressing ethical dilemmas and conflicts in patient care, rather than routine administrative tasks like granting access to medical records.
Choice B reason:
Asking the nursing supervisor to obtain the medical records for a family member is not appropriate without the client’s consent. Medical records are confidential and protected under laws such as HIPAA (Health Insurance Portability and Accountability Act), which require patient authorization for disclosure.
Choice C reason:
The healthcare provider cannot share medical information with a family member without the client’s explicit permission. This is to ensure the privacy and confidentiality of the client’s health information.
Choice D reason:
The correct procedure is for the client to provide permission to share their medical records. Under HIPAA, a healthcare provider can only share a patient’s medical information with family members if the patient has given explicit consent. This ensures that the patient’s privacy rights are respected and that their health information is protected.
Free Nursing Test Bank
- Free Pharmacology Quiz 1
- Free Medical-Surgical Quiz 2
- Free Fundamentals Quiz 3
- Free Maternal-Newborn Quiz 4
- Free Anatomy and Physiology Quiz 5
- Free Obstetrics and Pediatrics Quiz 6
- Free Fluid and Electrolytes Quiz 7
- Free Community Health Quiz 8
- Free Promoting Health across the Lifespan Quiz 9
- Free Multidimensional Care Quiz 10
View Related questions
Correct Answer is B
Explanation
Choice A reason:
The statement “This stage is when testing occurs to identify boundaries of interpersonal behaviors” describes the storming stage of group development. During the storming stage, group members test boundaries and challenge each other, leading to conflicts and disagreements.
Choice B reason:
The norming stage is characterized by the development of group cohesion and consensus. During this stage, group members start to resolve their differences, appreciate each other’s strengths, and work together more effectively. Consensus evolves as the group establishes norms and agrees on common goals.
Choice C reason:
While constructive efforts are part of the norming stage, the statement is too vague to indicate a clear understanding of this specific stage. Constructive efforts can occur in various stages of group development, including performing.
Choice D reason:
Resistance and the formation of subgroups are typical of the storming stage, not the norming stage. In the storming stage, conflicts and power struggles are common as group members assert their opinions and roles.
Correct Answer is C
Explanation
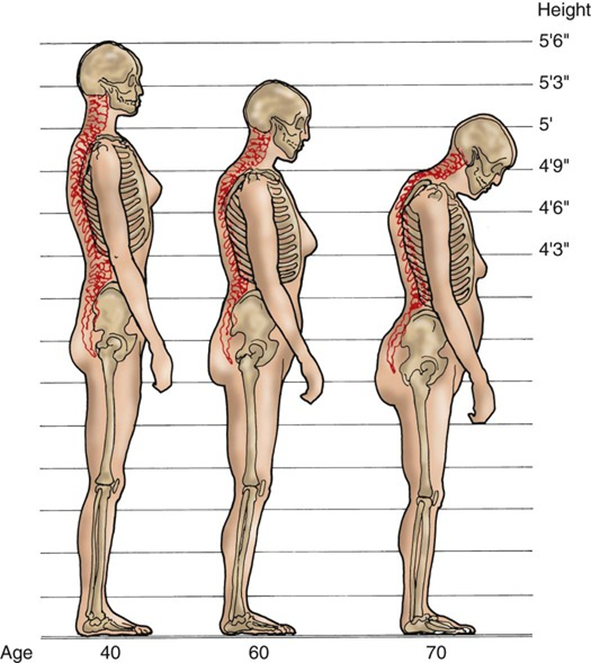
Choice A reason: Reduced chest width:
Aging does not typically result in a reduced chest width. Instead, changes in posture and the curvature of the spine can make the chest appear less prominent. The primary musculoskeletal changes with aging involve bone density, muscle mass, and joint flexibility.
Choice B reason: Increased force of isometric contraction:
This is incorrect. Aging is associated with a decrease in muscle strength and mass, not an increase. The force of muscle contractions generally diminishes with age due to the loss of muscle fibers and changes in muscle composition.
Choice C reason: Decreased muscle mass:
This is correct. One of the most significant age-related musculoskeletal changes is sarcopenia, which is the loss of muscle mass and strength. This process begins around the age of 30 and accelerates with age, leading to decreased physical strength and increased risk of falls and fractures.
Choice D reason: Thickened vertebral discs:
Aging typically leads to the thinning and dehydration of intervertebral discs, not thickening. This can result in a reduction in height and increased susceptibility to spinal issues such as herniated discs and spinal stenosis.