A nurse is caring for a client who has an extracellular fluid volume deficit. Which of the following findings should the nurse expect?
Dependent edema
Distended neck veins
Postural hypotension
Bradycardia
The Correct Answer is C
Choice A reason:
Dependent edema is not typically associated with extracellular fluid volume deficit. Edema usually occurs due to fluid overload or conditions that cause fluid retention, such as heart failure or kidney disease. In the case of extracellular fluid volume deficit, the body is losing more fluid than it is taking in, which would not result in edema. Instead, symptoms like dry skin, dry mucous membranes, and decreased skin turgor are more common.
Choice B reason:
Distended neck veins are also not a common finding in extracellular fluid volume deficit. Distended neck veins are usually seen in conditions where there is fluid overload or increased pressure in the venous system, such as heart failure or superior vena cava syndrome. In extracellular fluid volume deficit, the body is experiencing a reduction in fluid volume, which would not cause distended neck veins.
Choice C reason:
Postural hypotension, also known as orthostatic hypotension, is a common finding in extracellular fluid volume deficit. This condition occurs when there is a significant drop in blood pressure upon standing, leading to dizziness or lightheadedness. It is caused by the reduced blood volume, which decreases the amount of blood returning to the heart and subsequently lowers blood pressure.
Choice D reason:
Bradycardia, or a slow heart rate, is not typically associated with extracellular fluid volume deficit. In fact, the opposite is more likely to occur. Tachycardia, or a fast heart rate, is a common compensatory mechanism in response to fluid volume deficit as the body attempts to maintain adequate blood flow and pressure. Therefore, bradycardia would not be an expected finding in this scenario.
Free Nursing Test Bank
- Free Pharmacology Quiz 1
- Free Medical-Surgical Quiz 2
- Free Fundamentals Quiz 3
- Free Maternal-Newborn Quiz 4
- Free Anatomy and Physiology Quiz 5
- Free Obstetrics and Pediatrics Quiz 6
- Free Fluid and Electrolytes Quiz 7
- Free Community Health Quiz 8
- Free Promoting Health across the Lifespan Quiz 9
- Free Multidimensional Care Quiz 10
View Related questions
Correct Answer is B
Explanation
Choice A Reason:
A family whose only child recently died due to cancer is experiencing a significant and traumatic loss. This type of loss is categorized as a situational loss because it is unexpected and not part of the normal life cycle. Situational losses are typically sudden and can cause profound grief and disruption in the family’s life. The death of a child is one of the most devastating events a family can endure, leading to intense emotional pain and a long grieving process.
Choice B Reason:
A family whose oldest child is moving away for college is experiencing a maturational loss. Maturational losses are those that occur as part of normal life transitions and developmental stages. These losses are anticipated and expected as individuals grow and progress through different phases of life. The transition of a child moving away for college is a common maturational loss, as it signifies a significant change in the family dynamic and the child’s development into adulthood.
Choice C Reason:
A family whose house was destroyed in a fire is dealing with a situational loss. This type of loss is unexpected and can have a severe impact on the family’s sense of security and stability. The destruction of a home involves not only the loss of physical property but also the emotional attachment and memories associated with the home. Recovering from such a loss requires significant emotional and practical adjustments.
Choice D Reason:
A family whose head of household lost their job is experiencing a situational loss. Job loss can lead to financial instability and stress, affecting the entire family’s well-being. This type of loss is not part of the normal developmental process and can create significant challenges for the family as they navigate the uncertainty and potential changes in their lifestyle.
Correct Answer is A
Explanation
Choice A Reason:
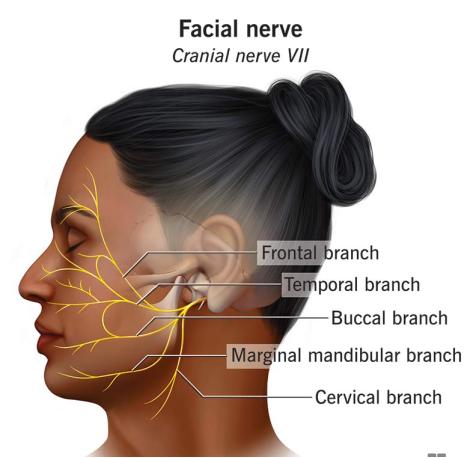
Cranial nerve VII, also known as the facial nerve, is responsible for controlling the muscles of facial expression. When assessing this nerve, a nurse would expect to see symmetrical facial movements, such as a symmetrical smile. This indicates that the facial nerve is functioning properly on both sides of the face. Any asymmetry could suggest a problem with the facial nerve, such as Bell’s palsy or a stroke.
Choice B Reason:
The position of the tongue is controlled by cranial nerve XII, the hypoglossal nerve, not cranial nerve VII. The hypoglossal nerve is responsible for the movements of the tongue, and a midline position indicates normal function of this nerve. Therefore, this response is not relevant to the assessment of cranial nerve VII.
Choice C Reason:
Turning the head against resistance is a test for cranial nerve XI, the accessory nerve. This nerve controls the sternocleidomastoid and trapezius muscles, which are involved in head and shoulder movements. Assessing the ability to turn the head against resistance helps evaluate the function of the accessory nerve, not the facial nerve.
Choice D Reason:
Pupillary constriction in response to light is a function of cranial nerve III, the oculomotor nerve. This nerve controls the muscles that constrict the pupil in response to light, a reflex known as the pupillary light reflex. This response is not related to the function of cranial nerve VII.