A nurse is attending a social event when another guest coughs weakly once, grasps his throat with his hands, and cannot talk. Which of the following actions should the nurse take?
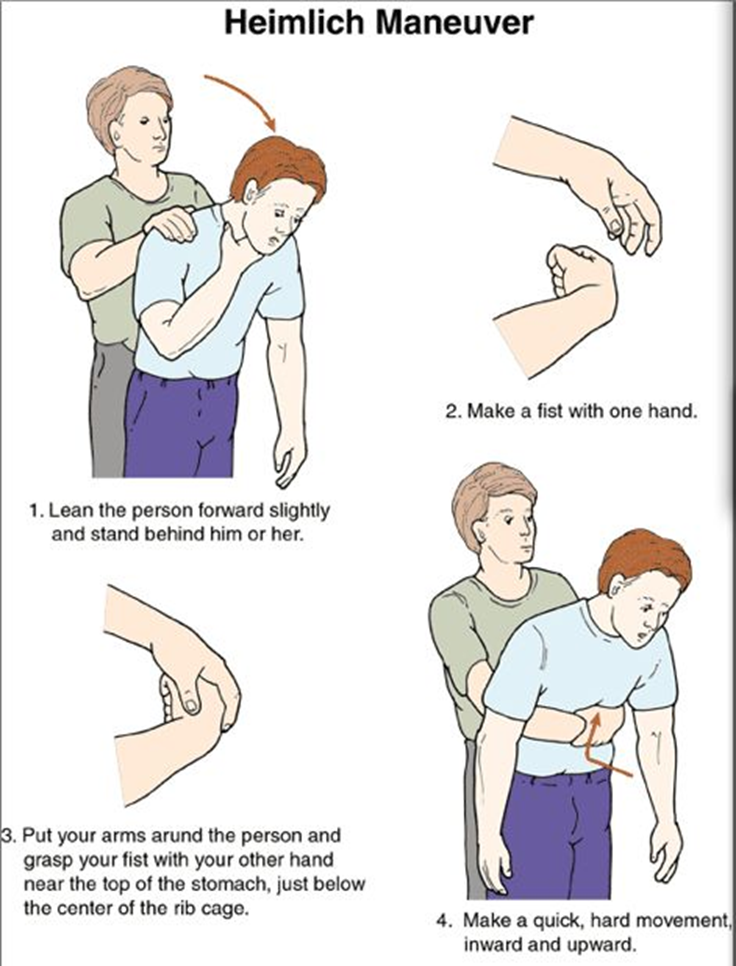
Perform the Heimlich maneuver.
Slap the client on the back several times.
Assist the client to the floor and begin mouth-to-mouth resuscitation.
Observe the client before taking further action.
The Correct Answer is A
Choice A reason:
The Heimlich maneuver, also known as abdominal thrusts, is the recommended first aid technique for a conscious person who is choking. This maneuver helps to expel the object blocking the airway by using the air remaining in the lungs to force it out. The nurse should stand behind the person, place their arms around the person’s waist, make a fist with one hand, and place it just above the navel. The other hand should grasp the fist, and quick, upward thrusts should be performed until the object is expelled.
Choice B reason:
Slapping the client on the back several times is not the recommended first action for a conscious adult who is choking. While back blows can be effective, they are typically used in combination with abdominal thrusts and are more commonly recommended for infants. For adults, the Heimlich maneuver is preferred as the initial response.
Choice C reason:
Assisting the client to the floor and beginning mouth-to-mouth resuscitation is not appropriate for a conscious person who is choking. Mouth-to-mouth resuscitation, or rescue breathing, is used when a person is not breathing and is unresponsive. In this scenario, the client is conscious but unable to speak, indicating a blocked airway that requires the Heimlich maneuver.
Choice D reason:
Observing the client before taking further action is not advisable in a choking emergency. Immediate intervention is crucial to prevent the situation from worsening. If the person is unable to speak, cough, or breathe, the Heimlich maneuver should be performed without delay.
Free Nursing Test Bank
- Free Pharmacology Quiz 1
- Free Medical-Surgical Quiz 2
- Free Fundamentals Quiz 3
- Free Maternal-Newborn Quiz 4
- Free Anatomy and Physiology Quiz 5
- Free Obstetrics and Pediatrics Quiz 6
- Free Fluid and Electrolytes Quiz 7
- Free Community Health Quiz 8
- Free Promoting Health across the Lifespan Quiz 9
- Free Multidimensional Care Quiz 10
View Related questions
Correct Answer is B
Explanation
Choice A: A Negative-Pressure Isolation Room
A negative-pressure isolation room is typically used for patients with airborne infections, such as tuberculosis, to prevent the spread of infectious particles through the air. Scabies, however, is spread through direct skin-to-skin contact or contact with contaminated items, not through the air. Therefore, a negative-pressure room is not necessary for a client with scabies.
Choice B: A Private Room
Placing the client in a private room is the appropriate action. This helps to prevent the spread of scabies to other patients and staff. Scabies is highly contagious, and isolating the affected individual minimizes the risk of transmission. The client should remain in the private room until the treatment regimen is complete and they are no longer contagious.
Choice C: A Semi-Private Room with a Client Who Has Pediculosis Capitis
A semi-private room with a client who has pediculosis capitis (head lice) is not appropriate. While both conditions involve parasites, they are different and require separate management and treatment protocols. Placing two clients with different contagious conditions in the same room increases the risk of cross-contamination and complicates infection control measures.
Choice D: A Positive-Pressure Isolation Room
A positive-pressure isolation room is used to protect immunocompromised patients from external contaminants by ensuring that air flows out of the room rather than in. This type of room is not suitable for a client with scabies, as it does not address the mode of transmission for this condition.
Correct Answer is A
Explanation
Choice A: Wrap the stump with an elastic bandage in a figure-eight configuration
Wrapping the stump with an elastic bandage in a figure-eight configuration is a standard practice in postoperative care for below-the-knee amputations. This method helps to shape and shrink the residual limb, preparing it for a prosthesis fitting. The figure-eight wrap provides even compression, which helps to reduce swelling and promote proper healing. It also helps to prevent the formation of edema and ensures that the residual limb maintains a conical shape, which is ideal for fitting a prosthetic socket.
Choice B: Remove the elastic bandage and re-wrap the stump once per day
While it is important to regularly check and adjust the bandage, removing and re-wrapping the stump only once per day may not be sufficient. The bandage should be checked more frequently to ensure it remains properly positioned and provides consistent compression. In some cases, it may need to be adjusted multiple times a day to maintain the desired level of compression and to prevent any issues such as slippage or uneven pressure.
Choice C: Perform passive range of motion exercises once daily
Performing passive range of motion exercises is beneficial for maintaining joint flexibility and preventing contractures. However, these exercises should be performed more frequently than once daily, especially in the early postoperative period. Regular exercises help to maintain muscle strength, improve circulation, and promote overall mobility. The frequency and type of exercises should be tailored to the individual needs of the client and guided by a physical therapist.
Choice D: Secure the elastic bandage to the lowest joint
Securing the elastic bandage to the lowest joint is not recommended. The bandage should be wrapped in a way that provides even compression without restricting movement or circulation. The figure-eight configuration is preferred because it allows for better control of the compression and helps to shape the residual limb effectively. Securing the bandage to a joint can lead to discomfort and may impede proper blood flow.