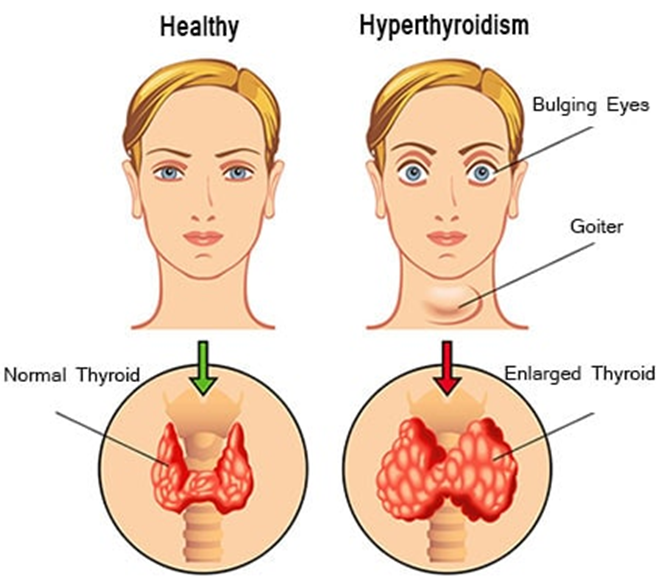
A nurse is assessing a client who has hyperthyroidism. The nurse should expect the client to report which of the following manifestations?
Constipation
Sensitivity to cold
Weight gain of 4.5 kg (10 lbs) in 3 weeks
Frequent mood changes
The Correct Answer is D
Choice A Reason:
Constipation is not typically associated with hyperthyroidism. Hyperthyroidism usually speeds up the body’s metabolism, leading to symptoms like increased bowel movements or diarrhea rather than constipation.
Choice B Reason:
Sensitivity to cold is more commonly associated with hypothyroidism, where the body’s metabolism slows down. In hyperthyroidism, patients often experience heat intolerance due to an increased metabolic rate.
Choice C Reason:
Weight gain of 4.5 kg (10 lbs) in 3 weeks is also more indicative of hypothyroidism. Hyperthyroidism generally causes weight loss despite an increased appetite because of the accelerated metabolism.
Choice D Reason:
Frequent mood changes are a common symptom of hyperthyroidism. The excess thyroid hormones can affect the nervous system, leading to symptoms such as anxiety, irritability, and mood swings.
Free Nursing Test Bank
- Free Pharmacology Quiz 1
- Free Medical-Surgical Quiz 2
- Free Fundamentals Quiz 3
- Free Maternal-Newborn Quiz 4
- Free Anatomy and Physiology Quiz 5
- Free Obstetrics and Pediatrics Quiz 6
- Free Fluid and Electrolytes Quiz 7
- Free Community Health Quiz 8
- Free Promoting Health across the Lifespan Quiz 9
- Free Multidimensional Care Quiz 10
View Related questions
Correct Answer is A
Explanation
Choice A: Decrease the Infusion Rate on the IV
Decreasing the infusion rate on the IV is the appropriate action to take when a client experiences flushing of the neck and tachycardia while receiving vancomycin. These symptoms are indicative of vancomycin flushing syndrome (VFS), also known as “red man syndrome,” which is a reaction caused by the rapid infusion of vancomycin. Slowing the infusion rate allows the body more time to metabolize the drug and can help alleviate the symptoms.
Choice B: Document that the Client Experienced an Anaphylactic Reaction to the Medication
Documenting that the client experienced an anaphylactic reaction is not accurate in this scenario. Vancomycin flushing syndrome is an anaphylactoid reaction, not an anaphylactic one. Anaphylactoid reactions are not mediated by IgE antibodies and do not require prior sensitization to the drug. Therefore, it is important to distinguish between the two and document the reaction correctly.
Choice C: Change the IV Infusion Site
Changing the IV infusion site is not necessary in this case. The symptoms of flushing and tachycardia are related to the rate of vancomycin infusion, not the site of infusion. Therefore, changing the site would not address the underlying issue.
Choice D: Apply Cold Compresses to the Neck Area
Applying cold compresses to the neck area may provide some symptomatic relief, but it does not address the root cause of the reaction. The primary intervention should be to slow the infusion rate to prevent further release of histamine and alleviate the symptoms.
Correct Answer is A
Explanation
Choice A: Obtain a 12-lead ECG
Obtaining a 12-lead ECG is a critical action when a client has a potassium level of 6.8 mEq/L, which indicates hyperkalemia. Hyperkalemia can cause serious cardiac dysrhythmias, including life-threatening arrhythmias such as ventricular fibrillation or asystole. An ECG can help detect these abnormalities early, allowing for prompt intervention to prevent cardiac complications. The ECG may show characteristic changes such as peaked T waves, widened QRS complexes, and prolonged PR intervals, which are indicative of hyperkalemia.
Choice B: Suggest that the client use a salt substitute
Suggesting that the client use a salt substitute is not appropriate in this situation. Many salt substitutes contain potassium chloride, which can further increase the potassium level in the blood. For a client with hyperkalemia, it is crucial to avoid additional sources of potassium to prevent exacerbating the condition. Therefore, recommending a salt substitute could be harmful.
Choice C: Advise the client to add citrus juices and bananas to her diet
Advising the client to add citrus juices and bananas to her diet is also inappropriate. Both citrus juices and bananas are high in potassium and can contribute to an increase in serum potassium levels. For a client with hyperkalemia, it is essential to limit dietary potassium intake to help lower the potassium levels in the blood. Encouraging the consumption of high-potassium foods would be counterproductive and potentially dangerous.
Choice D: Obtain a blood sample for a serum sodium level
While obtaining a blood sample for a serum sodium level can be part of a comprehensive assessment, it is not the immediate priority in managing hyperkalemia. The primary concern with a potassium level of 6.8 mEq/L is the risk of cardiac dysrhythmias. Therefore, obtaining an ECG to monitor the heart’s electrical activity is the most urgent and appropriate action. Once the immediate risk is addressed, further laboratory tests, including serum sodium levels, can be conducted as part of the overall assessment and management plan.